The game has now changed…with bonded restorations and new zirconia materials. Something as simple a creating an endo access hole now takes on a new dimension.
Whether digital or analog, when constructing single posterior crowns, we all have issues with “the bite.” I do not want to get into a detailed discussion of occlusion; dentists spend their careers taking courses in this area. Right now, I am talking to the practitioner who does a fair number of single crowns using triple or quadrant trays and gets a case back from the lab that required lots of time to grind it in. We have all seen too many cases with porcelain-fused-to-metal crowns where the metal bled through the occlusal. And we have all come up with a story to explain this “black spot” to our patients. Of course, it would be easy to reimpress, take a new bite or even modify the prep (or opposing teeth), and send it back to the lab, and many patients will accept this as they don’t pay as much attention as we do. Also, there is the time and cost to do this, as it requires another visit and, in some cases, a lab fee for adjustment. Also, patients often don’t want to come back and say things like, “It feels okay, and it’s good enough.” We have all been there, so be sure to put copious notes in the chart documenting the situation and discussion.
Then we run into situations where things were fine, but the patient returns and complains about a problem with that crown. Some things are adjustable dentally (or mentally), and others will require a remake. Now you must numb that patient, cut off the crown, re-prep, and take new impressions. One of my dental school instructors had many sage sayings, one of which was “If you don’t have time to do it right the first time, you will never have time to do it over.” In the days we were cementing gold, PGC, and other restorations, all we had to do was make a few slots and pop off the crown. There is a wonderful instrument available from GoldenDent (makers of Physics Forceps) called the WAMkey. It is a very simple device, resembling a thin screwdriver, that requires you to merely make a slot in the buccal of the tooth, slip in the right size (there are 3), and give it a twist. The patients don’t realize that you removed it, as there’s no tugging or twisting and flying porcelain. There is a minor learning curve on how to angle the slot, but there are clear instructions (be sure to read them) and videos. This device is also helpful in removing a bridge and—in a few cases, if you are careful—the buccal can be repaired, and in cases where there was a loose abutment, at least the bridge can go back as a temporary, but assume you are remaking it.
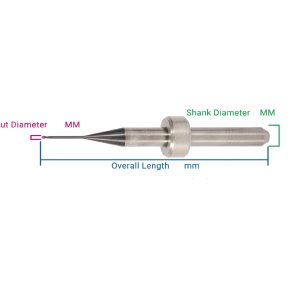
The game has now changed, though, with bonded restorations and new zirconia materials. Something as simple as creating an endo access hole now takes on a new dimension. You can cut slots in these, but when you try and twist them off, they don’t always go. And with other bonded restorations, such as IPS e.max (Ivoclar Vivadent) or some of the CAD composite blended ceramics, the bonds are better and you could twist off part the of prep, or, in some cases, you are forced to prep off the crown and cement. Luckily, there are new burs that have come out specifically designed to cut into or remove zirconia. All diamond companies now sell these FG diamonds along with zirconia polishers, which usually have latch attachments. (This is a good argument for discussing electric handpieces, which will be done another day.) According to the experts, it is critical to polish zirconia restorations after any occlusal adjustment or risk damage to the opposing teeth. There have been many articles by both clinicians and labs, as well as by polisher manufacturers, outlining the steps to bring the surface back to smooth.
One common cause of this issue is insufficient occlusal preparations. We often find this out when constructing a temporary. Everything seemed okay visually when checking the clearance, but, when making the temp, we find an area with a hole or paper-thin material. At this point, the patient is ready to leave and not very interested in hearing you say you have to “do a little more and take just one more impression.” Many tend to write a lab instruction to “spot the opposing” or “send a reduction coping.” With a vital tooth, the latter is a challenging process without using local anesthetic, and for those of you who have done this, it is not terribly accurate. To make things worse, many lab slips have this issue pre-printed, ie, they know it is an ongoing issue.
What is the purpose of this whole discussion? It adds more fuel to the decision to switch to digital impressions. First of all, most of the programs tell you with text or colors that you do not have enough room for the material you have chosen. Second, if you have to change your prep after you took the impression, you merely digitally erase the prep from the scan, reduce the area, and just rescan the tooth. The total time is less than 30 seconds and of no inconvenience to the patient. Plus, with a digital bite, you can see the patient fully closed and in centric. There is no triple tray or bite material to look through and no more notes to the lab saying “The patient bit wrong.” (Note: Kettenbach LP’s new Futar Clear Fast bite material helps this situation.) Next, the case comes back with centric, and all you may have to adjust are lateral excursions, thus reducing seating time, a true ROI. So, what about lateral excursions in the digital world? Stay tuned for my column on virtual articulation, essentially using the patient’s TMJ as the articulator.